
Common Disorders We Treat
- Club foot
- Flat foot
- Accessory Navicular
- Tarsal coalition
- Osteochondritis dissecans
- Osgood Schlatter disease
- Hip dysplasia
- Perthes disease
- SCFE
- Congenital Muscular Torticollis
- Bow legs (Genu varum)
- Knock knees-Genu valgum
- Pediatric fractures
Club foot
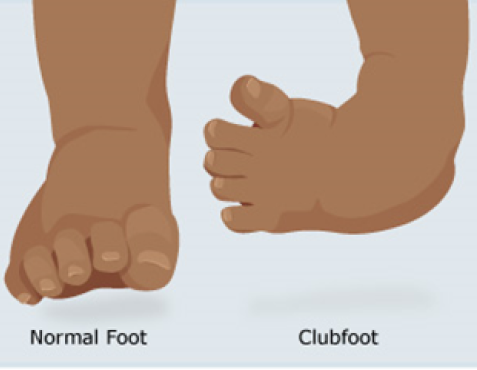
Clubfoot is a condition in which a child is born with one foot or both feet turned inward (misshaped). It is important to start treatment within 1-3 weeks after birth. The goal of treatment is to straighten the foot so your child can stand or walk painlessly with the sole of the foot flat on the ground. The foot shape can usually be corrected with stretching, casting, and bracing. In rare cases, surgery is needed.
Flat foot
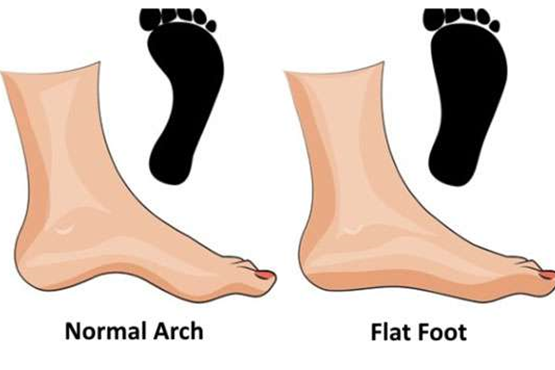
Flat feet are a common condition, often runs in families and is usually painless. In some cases, flat feet can affect the body’s alignment, which can cause knee and ankle discomfort. For children who are experiencing pain associated with their flat feet, doctors may recommend a variety of non-surgical treatments to relieve the pain, including arch supports, supportive shoes, stretching exercises, physical therapy and rest. Surgery is not usually needed for flexible flat feet but those with fixed flatfoot in conditions such as Tarsal coalition, surgery may be recommended.
Accessory Navicular

The accessory navicular is an extra bone or piece of cartilage located on the inner side of the footj ust above the arch. It is incorporated within the posterior tibial tendon. An accessory navicular is congenital (present at birth). Adolescence is a common time for the symptoms to first appear. Symptoms include vague pain that usually occurs after a period of activity. Non-surgical treatment include immobilisation, ice, medications, physical therapy and orthotics. Surgery may involve removing the accessory bone, reshaping the area and repairing the posterior tibial tendon to improve its function.
Tarsal coalition
A tarsal coalition is an abnormal connection between two or more of the tarsal bones in the foot. The chief symptom of tarsal coalition is pain starting in late childhood or early adolescence. Symptoms include rigidity and stiffness in and around the ankle with decreased range of motion. Non-surgical treatment aims to reduce the pain and muscle spasms and include casts or walking boots; orthotics; injection of an anaesthetic and a steroid for temporary relief; anti-inflammatory medications; stretching and physical therapy. When conservative therapy fails surgery is recommended which includes resection of the tarsal coalition replaced with fat or muscle.
Osteochondritis dissecans
Osteochondritis Dissecans is a condition in which a small segment of bone in a joint begins to separate from its surrounding region due to a lack of blood supply, most often in children and adolescents. The most common joints affected by osteochondritis dissecans are the knee, ankle and elbow. The OCD lesions can even detach and float around inside the joint. Symptoms of OCD include pain and swelling of a joint often brought on by sports or physical activity. Advanced cases of OCD may cause joint catching or locking. In most cases, OCD lesions in children and young teens will heal on their own. Surgical treatment is indicated when non-surgical treatment fails; lesion detaches and move around in the joint; lesion is very large (>1cm in diameter).
Osgood Schlatter disease

Osgood-Schlatter disease is a condition that causes pain and swelling below the knee joint, where the patellar tendon attaches to the top of the shinbone (tibia). It is most commonly found in young athletes who play sports that require a lot of jumping and/or running. It is caused by irritation of the bone growth plate by the prolonged stress. Activities that put stress on the knee—especially squatting, bending or running uphill can cause the tissue around the growth plate to hurt and swell. The disease usually goes away with time and rest. The appropriate time to return to sports will be based on the athlete’s pain tolerance. Surgery is recommended only if there are bone fragments that did not heal.
Hip dysplasia
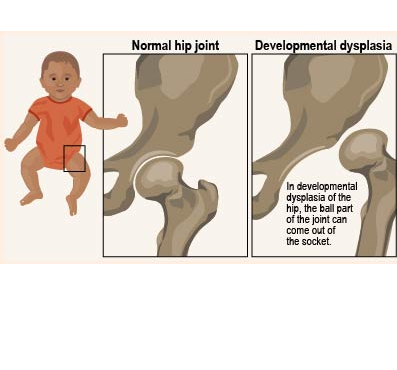
DDH is a condition in which the femoral head has an abnormal relationship to the socket (acetabulum) as a result of improper development of the hip ball and socket joint. The severity may vary from mild dysplasia to frank dislocation of head out of the socket. Causes of hip dysplasia can be due to frank breech delivery, ligamentous laxity or extended hip position in post-natal period.Symptoms include child walking with toe touch due to shortening of the limb. In 1 to 6 months of age, conservative treatment is advised in the form of pavlik harness. In 6 to 18 months old child, traction and closed reduction with hip Spica is given for 3 months. If reduction fails, open reduction is recommended. In 18 to 24 months of age, trial of closed reduction or primary open reduction is advised combined with acetabular osteotomy surgery like Salter’s osteotomy. In older child, femoral shortening is used along with above procedures to put less pressure on femoral head after reduction. Early detection and timely intervention are both important to reduce a child’s risk of pain and disability in adulthood.
Perthes disease
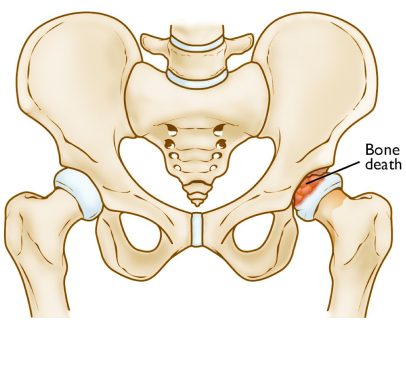
Perthes disease is a rare childhood condition of hip. It occurs when the blood supply to the head of the femur (thighbone) is temporarily disrupted. Without an adequate blood supply, the bone cells die. Perthes is really a complex process of stages that can last several years. As the condition progresses, the weakened bone of the head of the femur gradually begins to collapse. The goal of treatment is to relieve painful symptoms, protect the shape of the femoral head, and restore normal hip movement. If left untreated, the femoral head can deform and not fit well within the acetabulum (hip socket), which can lead to further hip problems in adulthood, such as early onset of arthritis.
Treatment plan is based on the age of the child and extent of disease involvement. For very young children (2 to 6 years of age) with few changes in the femoral head on x-rays, conservative management is advised in the form of observation, anti-inflammatory medications, physiotherapy and life-style modifications. For older children with more than 50% involvement of the femoral head, surgery is recommended in the form of osteotomy +/- femoral shortening in which bone is cut and repositioned to keep the femoral head snugly in the acetabulum.
SCFE
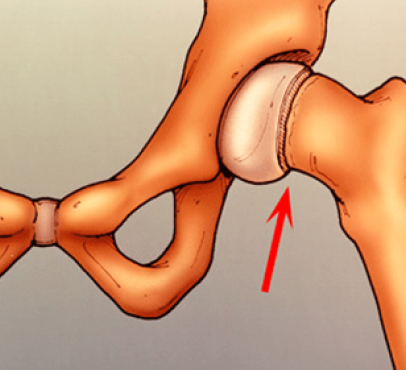
This condition most often affects the hip in teenagers between the ages of 12 and 16. The condition refers to the slip of the growth center of the hip on the top of the femur bone. Children who are overweight are more prone to developing SCFE. Most teenagers with SCFE develop pain in the hip, and they begin to walk with a limp. The condition can be treated and the complications avoided or reduced if recognized early. Surgery is usually necessary to stabilize the hip and prevent the situation from getting worse.
Congenital Muscular Torticollis
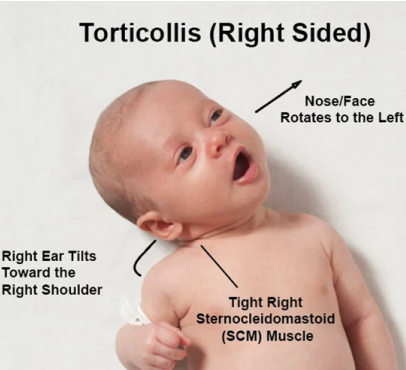
The term torticollis means “twisted neck”.CMT occurs when there is increased tone of the muscle called sternocleidomastoid (SCM) on one side. Causes include ischaemia, trauma during childbirth, intrauterine malposition. Child presents with lateral bending of neck towards the affected side. Conservative management include physiotherapy and manual stretching. Surgical management is done in case of no improvement with manual stretching. Options include unipolar/ bipolar SCM muscle lengthening, ‘z’ lengthening.
Bow knees-Genu varum

Genu varum is an angular deformity of the knee in which the child appear ‘’bowlegged’’. Varus is physiological in children aged 6 to 12 years and considered abnormal after 2 years. Pathological causes of genu varum include blount’s disease, nutritional rickets, post traumatic, congenital deformities, fibrous dysplasia. In late adulthood it can progress and lead to osteoarthritis. Children with physiological varus are managed by educating and reassuring the parents. In older children with pathological varus progressively increasing with age, operative treatment is done in the form of tibial osteotomy, femoral osteotomy or guided growth.
Knock knees-Genu valgum
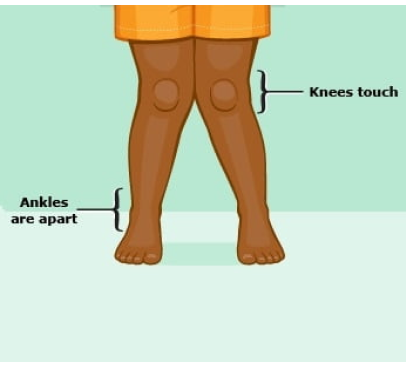
Genu Valgum is a condition in which knees are deviated towards midline of the body and both knees touch each other when straightened. Physiological genu valgum is present in children upto 4 years. Unilateral genu valgum can be seen in physeal injury, proximal metaphyseal fractures, benign tumour. Both sides genu valgum can be caused by renal osteodystrophy or skeletal dysplasia. Non operative treatment is advised in physiological genu valgum in children < 6 years, or treatment of the underlying primary cause. Operative treatment can be done in the form of hemiepiphysiodesis, bone stapling and corrective osteotomy in older children not responding to conservative treatment.
Pediatric fractures

Pediatric fractures are breaks in bones that occur in children, commonly due to falls, sports or accidents. Because children’s bones are still growing, they can heal more quickly and often more completely than adult bones. Common types include buckle, greenstick, and growth plate fractures. Symptoms include pain, swelling, bruising, and difficulty using the affected limb. Treatment typically involves immobilization with a cast or splint, and in some cases, realignment or surgery may be necessary. Prompt medical evaluation is essential to ensure proper healing and to avoid growth disturbances.
